Pudendal Neuralgia
Hello, Bestie, glad you’re here. We haven’t talked about pelvic pain for a little while, so I thought it would be a good idea to revisit one of my favorite pelvic pain topics: pudendal neuralgia. At first glance/read, “pudendal neuralgia” is giving me big “what the bean is that?” vibes. And for good reason. It’s one of those diagnoses that we don’t really have a layman’s term for. So, let’s break it down.

Pudendal Nerve
The pudendal nerve is one of the nerves responsible for sensation and function in your pelvic region. The word “pudendal” actually comes from the Latin word “pudendum” meaning “thing to be ashamed of.” The origins of the term are deeply connected to ancient times and it’s pretty wild that the external genitalia were literally named after the feeling of shame they invoked at the time. Also, how nuts is it that we often still associate feelings of shame and discomfort with the external genitalia in this day and age! Have you seen that trend where ladies ask guys how often they think about the Roman Empire? And according to most guys, they think about it all the time? Well, turns out I also think about the Roman Empire all the time, except I’m just fuming over them using the word for “shame” to name women’s genitals. Okay, back to business.
So, now that we know what “pudendal” means (even though we’re not happy about it), let’s talk about the term “neuralgia.” Neuralgia is nerve pain. It is the type of pain that typically feels like shooting, burning, tingling, or really any kind of altered sensation. So pudendal neuralgia, simply put, is pain in the pudendal nerve.
What does the pudendal nerve innervate?
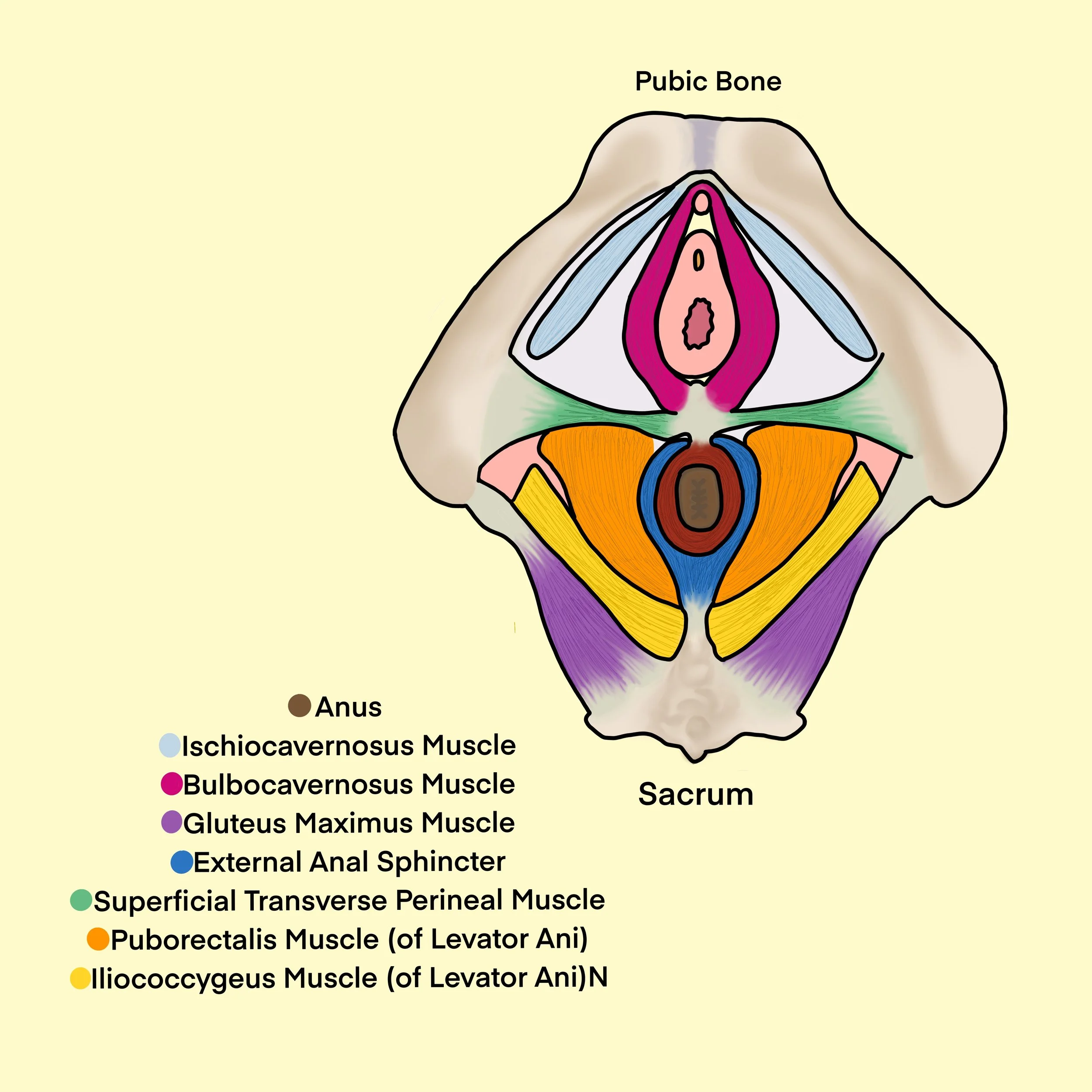
All nerves supply energy to specific parts of the body. This is called “innervation.” As discussed, the pudendal nerve is a nerve that innervates areas of the pelvic region. So, which areas are we talking about? Well, the pudendal nerve actually splits into three separate branches. Each of these branches innervates different parts of the pelvic region. The first branch is called the inferior rectal nerve. This nerve provides sensation to the skin around the anus and it allows the external anal sphincter muscle to be able to contract and relax. The second branch is called the perineal nerve. This nerve provides sensation to the area between the vulva/scrotum and the anus, as well as some sensation to the skin of the scrotum and labia majora. It also provides motor innervation to many muscles including the superficial transverse perineal, bulbocavernosus, ischiocavernosus, levator ani, and more. If you’re a little lost and need a review of the muscles of the pelvis, check that out here. The third and final branch of the pudendal nerve is called the dorsal nerve to the clitoris/penis (depending on the anatomy present). This nerve is responsible for erection.
What causes pudendal neuralgia?
Pudendal neuralgia may be caused by a variety of things such as, but not limited to pelvic surgery, childbearing, cycling, prolonged sitting, constipation, anal intercourse, pelvic trauma, and more.
What are the symptoms of pudendal neuralgia?
Symptoms of pudendal neuralgia include pain in the region innervated by the nerve. Often times, pain is worse with sitting, due to the compression on the nerve, but improves when sitting on a toilet, since the toilet is open and there is less compression over where the nerve runs. Typically, the pain caused by an issue with the pudendal nerve does not cause folks to wake up at night. Patients often describe burning, shooting, or tingling pain, or numbness. The pain usually presents on one side, rather than both and will be tender when your provider touches the area near your sits bones. Since the pudendal nerve splits off into other branches, if the pudendal nerve is implicated, it means those subsequent branches may not be able to perform their jobs either. This could result in symptoms such as erectile dysfunction.
How is pudendal neuralgia treated?
Pudendal neuralgia may be treated with a variety of methods, and, once again, the best results will come from a treatment plan that is broad and specifically tailored to you and your symptoms. Medications may be prescribed by your physician to treat symptoms associated with pudendal neuralgia. These can include muscle relaxants (Valium, Baclofen), tricyclic antidepressants (Elavil), topical anesthetics (lidocaine jelly), and more. Other treatments include steroid injections near the pudendal nerve and potential decompression surgery to free the pudendal nerve from being squished (1).
In physical therapy, your pelvic health specialist can work with you using various treatment techniques including massage, nerve mobilizations, and desensitization. Your therapist might also teach you how to support your perineum and pudendal nerve during bowel movements to avoid unnecessary stretching of the pudendal nerve that could be aggravating. You will learn which stretches can be helpful and which to avoid. It is important to avoid aggravating activities when possible. Other things that could come up in treatment include addressing pelvic floor muscle (PFM) tension, application of cold or warm compresses, electrical stimulation, and discussions on positioning (sitting and lying down) for comfort.
Here’s the bottom line: if you have been suffering from pelvic pain, it could be a result of pudendal neuralgia! Talk with your healthcare provider about your symptoms so that you can get to the bottom of what’s causing your pain. If you have pudendal neuralgia, know that there are tons of treatment techniques that could work for you and your healthcare providers should work with you to determine the best fit.
Now remember, there’s no shame in pudendal neuralgia—well, technically there is—but there shouldn’t be, and there’s definitely no shame in getting it treated! Here’s to being shameless.
XOXO,
Your Pelvic Bestie
References:
1. Itza Santos, F., Salinas, J., Zarza, D., Gómez Sancha, F., & Allona Almagro, A. (2010). Update on pudendal nerve entrapment syndrome: an approach anatomic-surgical, diagnostic and therapeutic. Actas Urológicas Españolas (English Edition) , 34 (6), 500– 509.
*The information contained in this article is for educational and informational purposes only and is not intended as health or medical advice. Always consult a qualified health provider regarding any questions you may have about a medical condition or health objectives.